Understanding the process of wound healing is critical to optimal outcomes for any patient with a surgical wound. In essence, when skin edges are brought together with sutures after surgery, a fibrin gel acts as an initial sticky gel to help the opposing tissues adhere to each other. Over the subsequent 3-4 days new capillary blood vessels grow out from the wound edges to link the incision edges. Collagen is then produced by fibroblasts within this portion of the wound. The word collagen is derived from the Greek term kolla, meaning glue.
Whilst the sutures (stitches) placed by the surgeon securely approximate the skin edges, it is the maturing collagen that provides the real sustaining strength in the repaired wound. The strength of this repair does however take time to develop varying according to many factors including the site, tension across the repaired wound, and the quality of blood supply (and thereby nutrition) of the wound. Depending on these factors, the wound support by the sutures is critical for periods that may vary from 5 days to over 3 weeks.
Surgical wounds can be closed by a very varied combination of both internal (absorbing) and external stitches (that need to be removed). A wide range of factors influence the decision as to how a wound is closed. The technique of wound closure needs to be discussed with all patients immediately after surgery as it frequently has a major impact on how patients should care for their wounds.
Conventional sutured wounds
These wounds, whether undertaken as simple procedures under local anaesthetic, or as more significant operations including flaps performed in an operating room are all appropriately cared by the following;
Flap Repairs
Wounds repaired with flaps generally cared for in much the same way as described above. Conceptually, a flap can be thought of as the transfer of skin from area of relative laxity (tissue abundance) into a defect (typically after skin cancer removal or a trauma defect). The transferred tissue is nourished by an underlying blood supply (tissue bridge) that is is transferred along with the skin. Because all the skin is vascularised wound healing is typically reliable and wound care simple. Some examples of commonly used flaps and their healing/wound care are illustrated below.
Bilobed flap repair after excision of a basal cell cancer on the nasal tip

The visibly apparent skin cancer (BCC) is outlined with dotted marks and the actual excision and planned flap (transfer of skin) indicated by the heavy blue line above.

Wound 7 days after surgery.
Wound care has consisted of normal showering and simple application of an antibiotic ointment once a day from the first post-operative day. Sutures are typically removed 6-8 days later.

Wound immediately after suture removal.

Wound 3 weeks after surgery. Scars vary greatly with every patient but always progressively improve for many months.
Scalp Rotation Flaps are used when ever possible to repair scalp defects as they provide optimal cosmetic repairs and are very easy to care for post-operatively.

The pre-invasive melanoma is delineated by the dotted outline. The planned excision and flap repair is drawn.

10 days post-operatively the wound is ready for the staples to be removed. Wound care has simply consisted of showering to wash the wound from the first post-operative day.
Keystone Flaps are commonly used to repair larger excision defects and are especially useful on the limbs as they can often obviate the need for a skin graft. This allows for a more rapid recovery, superior aesthetic appearance, and substantially less complex wound care.

The planned excision and modified keystone flap repair of an early melanoma on the lower leg has been planned.

Sutured wound at the end of the surgery.

Appearance of wound 1 week post-operatively. Wound care has simply consisted of gentle washing during normal daily showering and the application of a small amount of Betadine/antiseptic solution daily. A small amount of resolving bruising is apparent. Sutures are typically removed after 3 weeks.

Another keystone flap on the lower leg approximately 5 months post operatively
Skin Grafts
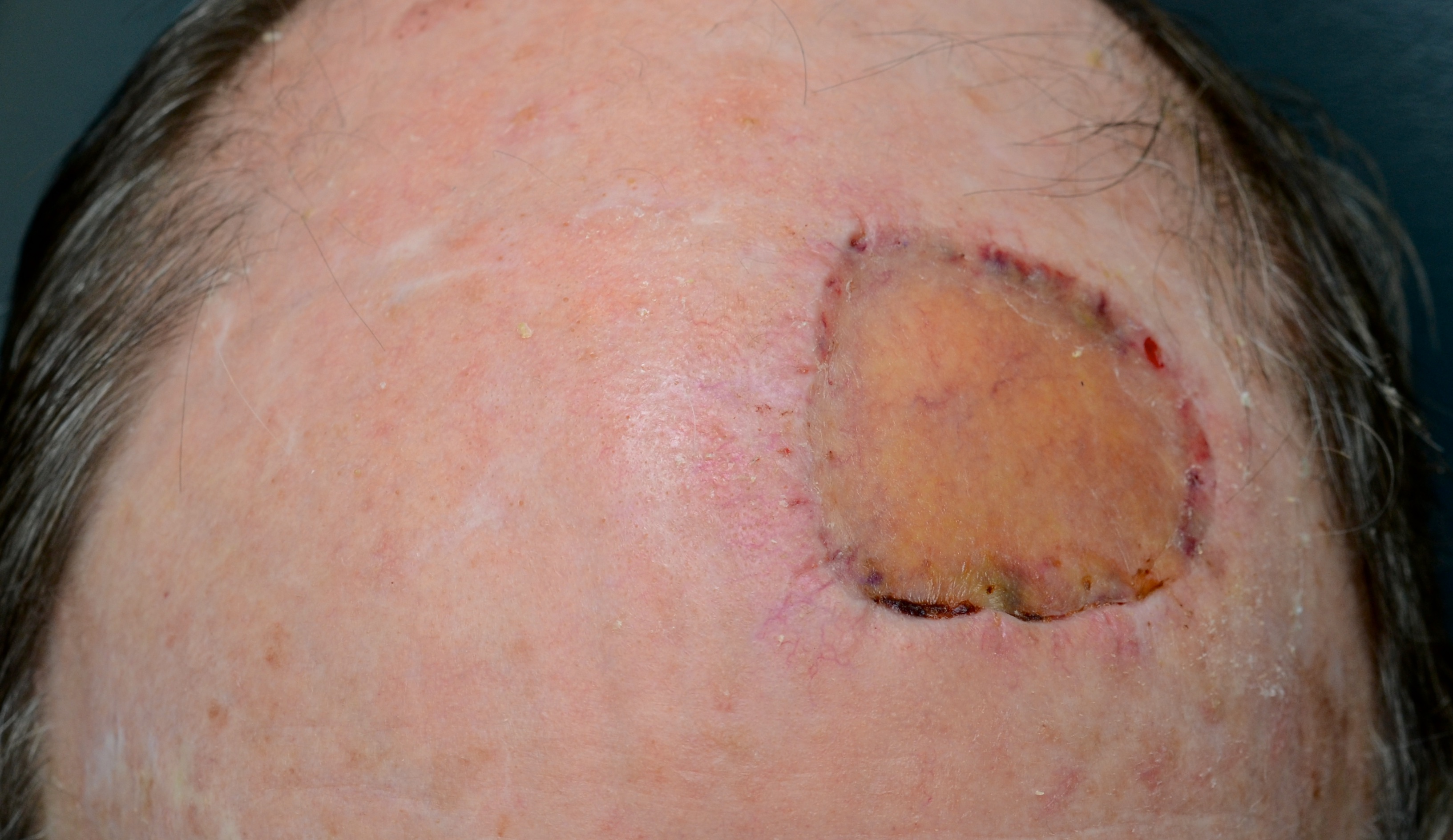
Full thickness skin grafts are ofter used to repair wounds on the face. A piece of skin with appropriate characteristics (texture, colour, thickness) is obtained from a donor site that can itself be closed directly with sutures and is usually located at a relatively inconspicuous site. The graft is then carefully secured into the original wound (usually the site of a skin cancer excision or an injury when skin has been lost). The dressing is designed to encourage blood vessels in the base of the defect to grow into the graft. The initial process of graft vascularisation typically takes 7-10 days and it is highly desirable that the graft is held securely against the wound base.

A diffuse area of pre-invasive melanoma and planned excision.

Skin graft has been secured beneath a foam pack to immobilise it against the excision defect.

10 days post-operative. The stabilising foam dressing has been removed and the skin graft has established a very significant blood flow/circulation.
Another week later and the blood flow through the skin graft has returned to more normal levels and is hence less red.

6 weeks post-operatively the skin graft continues to heal very well. The graft has significantly increased in bulk.
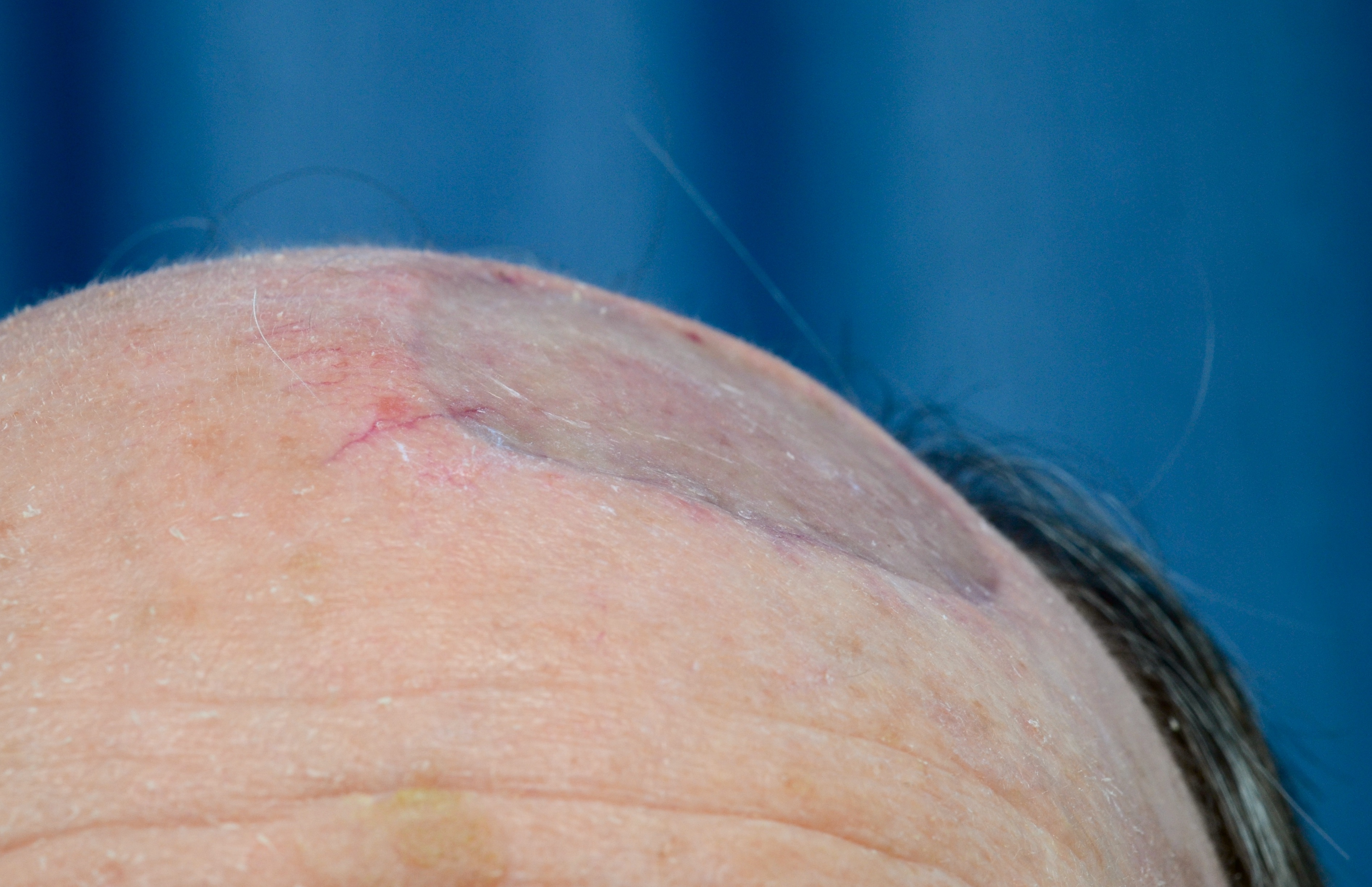
The repaired defect has a progressively decreasing contour defect as the graft incorporates. This is a particular quality of full thickness skin grafts compared to thinner split thickness skin grafts.
Split (partial thickness) Skin Grafts
Larger excision defects and trauma wounds may not be suitable for repair with either flaps or full thickness skin grafts. In these instances a skin graft consisting of only a portion of the skin may be the most appropriate way to repair the defect. These grafts are generally reliable but issues such as vascular disease, diabetes, pre-existing infections, and wound sites on the lower limb can present challenges.

Excision of an extensive but fortunately superficial melanoma on the forearm is planned.

A sheet of split thickness skin has been harvested throw the patient’s thigh and secured into the excision defect. Numerous small perforations have been in the graft to prevent fluid collecting between the graft and the base of the wound.

At the end of the surgery the graft is secured beneath a foam pack.

7 days post-operatively the foam pack has been removed.
The skin graft has developed a good blood supply from the underlying wound base. At the periphery of the graft, where it overlaps the underlying skin edges, the graft has desiccated. This is entirely normal and simply trimmed.

A week later the skin graft is more mature and incorporating extremely well. Over the coming weeks the graft will thicken and the contour